Intermittent Fasting Isn't Special
Why intermittent fasting is probably about as good as any other form of calorie restriction.


Diet culture is a fascinating beast. Most people in the diet world are convinced that there is one highly-specific way to lose weight and feel good about yourself—usually it’s the one that worked for them—and they will sell it to you as part of an online course with a free recipe book included in the price. Sometimes they also sell handy supplements to go along with the course that really work.
The reason this is all so interesting is because it conflicts so much with the data. If you look at the scientific literature, there isn’t really a “best” diet. In theory there are some advantages for various diets over others—low-carb has theoretical advantages for people with diabetes, DASH the same for people with heart disease—but when it comes to the real world it’s all a wash.
The problem is that this fairly well-demonstrated fact does not sell many diet books. It’s why I’ve had two agents turn down my book idea, which is to lay out the scientific evidence that most diets are about the same for your health. No one wants to hear that there are no silver bullets, they want the silver bullets because otherwise everything is just so much harder for us all.
Which brings us to intermittent fasting (IF).
If you listen to some of the online gurus, IF is magical. It’s not just a way to lose a few pounds/kilos, it’s a remarkable way to reset your very cells and extend your lifespan. The idea of the diet is simple—you just restrict your eating either by skipping meals or having very low calories on certain days—but this can apparently transform your life.
Except, the data is not nearly so simple.
The Science
The newest study to look at IF is an updated Cochrane systematic review. This is a type of study where researchers comb the literature looking for all of the studies conducted on a topic. In this case, they looked for randomized clinical trials that lasted at least 6 months comparing IF to other diets or a control group with no diet advice, and aggregated all of the trials together to look at the overall effect.
Cochrane reviews are generally considered the gold standard in medical evidence. The Cochrane Collaboration has a name for reliability and robustness, which they’ve earned through diligence and hard work. The main complaint that people have about Cochrane reviews is that they can be too careful, which has its own problems.
This particular review identified 22 randomized trials that fit the bill, with 1,995 total participants across the papers. To give you an idea of what the results look like, here’s a graph from one of the primary analyses:
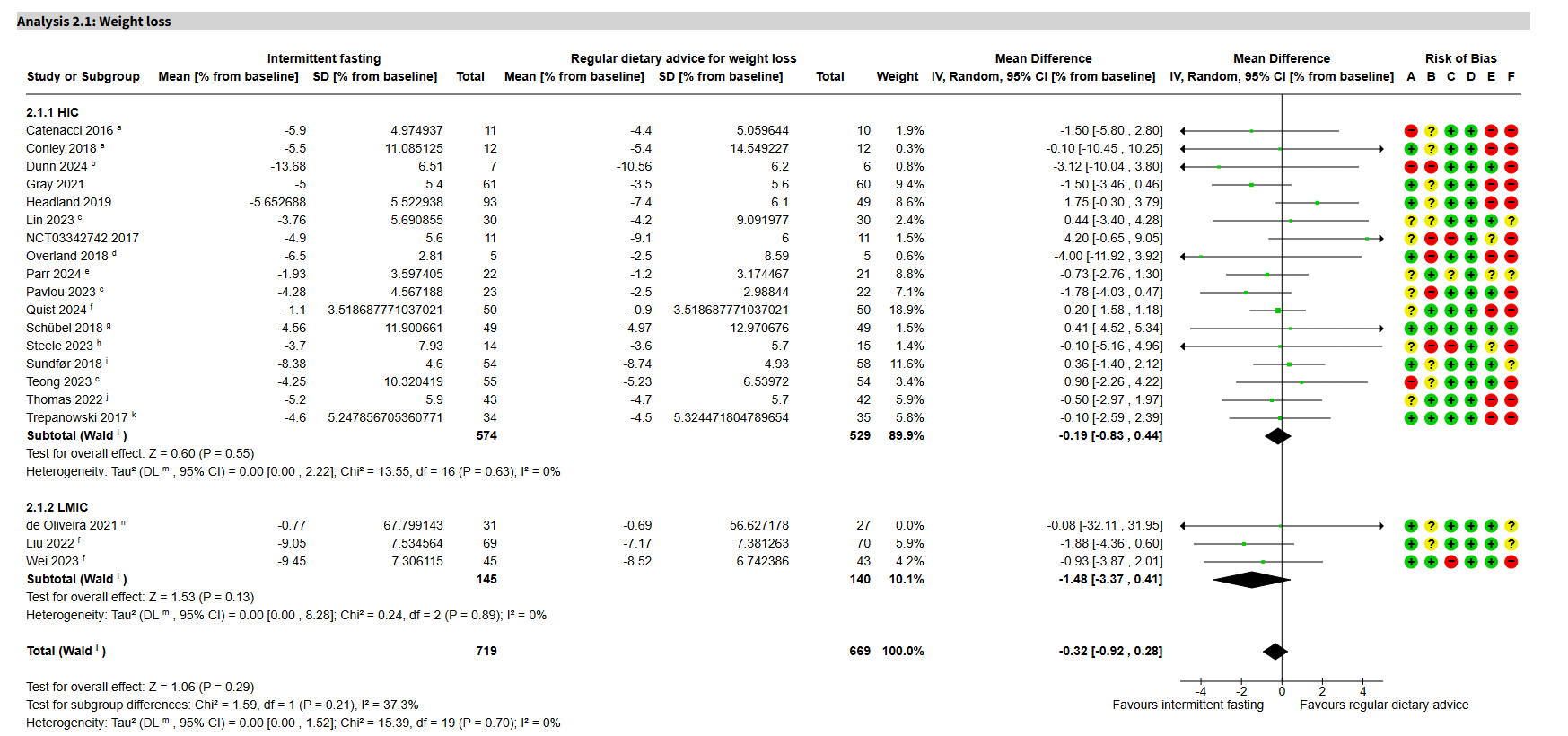
This is a bit complex, so let me explain. The column on the far left lists the studies, broken up into High-Income Countries (HIC, mostly EU and US) and Low/Middle-Income Countries (LMIC, Brazil and China). Next come columns that show the estimates of effect—the average change in weight—for the IF and control groups. Then you get the mean difference column, which shows the average difference between the IF and control group for each study. The mean differences are then shown as points with confidence intervals, which is the bit with the horizontal lines with arrows on what’s called a forest plot. The black line running down the middle of those horizontal lines is at the null point—this means that a study sitting on that black line has shown no difference between the IF and control groups.
Finally, we’ve got the risk of bias column. This is a rating that the Cochrane review authors give to each study that indicates how reliable they think it is. A study with all green is considered reliable, green and some yellow is mostly reliable, and any red means that the study is likely to be unreliable.
There are two key takeaways here. Firstly, the diamonds. If you look at the bold black diamonds in the forest plot—the bit with the horizontal lines—you can see that those diamonds are basically on the null point line. These diamonds represent the average effect of all of the studies, which means that this statistical model with all of these randomized trials shows no benefit for IF when compared to regular dietary advice.
The other important point is the risk of bias. There are very few trials with only green or green and yellow in the risk of bias column, which means that we are not certain about the overall model. However, if you look at just the reliable papers, they seem to be consistent with the overall estimate, which is to say that the highest-quality research seems to show no benefit for IF when compared to regular dietary advice.
The Cochrane review authors did this sort of statistical model for dozens of outcomes. They looked at what happens if you divide the studies into men and women, high-income vs low-income, and other sensitivity analyses. Across all of these, there were no benefits for IF on any measure when compared to regular dietary advice.
The only thing that IF appeared to be a little bit better than was no no diet at all. Compared to not going on a diet, IF reduced weight by around 3kg over six months.

Basically, IF worked no better than just telling people to eat a bit less food in randomized studies that had 6 months or more of data
. As with all reviews, the devil is in the detail. The Cochrane authors did a good job, but are the included studies worth relying on?
In my opinion, the Cochrane ratings are mostly quite fair. I didn’t read all of the papers, but the ones I looked over—and the ones I’ve read in the past—are pretty much in line with what the Cochrane reviewers thought of them. Most of the research was relatively unreliable, with a few quite strong studies in the mix. For example, one of the most robust papers was this German study comparing IF to caloric restriction and a control group who didn’t diet. At 12 months, they found no difference between IF and caloric restriction on any metric that they tested. There are always things to quibble about, but as far as I can tell the conclusions of the Cochrane authors are very reasonable:
“Compared to traditional dietary advice (like restricting calories or eating different types of foods), intermittent fasting may make little to no difference to weight loss and quality of life in adults living with overweight or obesity.”
Whatever Diet Works
This is yet another story of how most diets are basically the same when real people try them in their day-to-day lives. IF has all sorts of potential theoretical benefits—although many of these are somewhat dubious as well—but in practice real people don’t lose more weight or get healthier when you tell them to use IF than they would if you just told them to restrict their calories.
This is true for every diet I’ve ever come across. Low-carb is similar to high-carb as long as the calories are the same. Veganism has no major benefits over keto as long as you manage your cholesterol. As far as weight loss and general health goes, IF appears to be about as good as every other diet that we’ve ever looked into.
Personally, I’m a big fan of IF. It’s what I do to maintain my weight. I’ve tried many other dietary patterns but I’ve stuck with IF because it fits into my life quite neatly. But I know many people for whom it doesn’t seem to work, which is rather similar to what the evidence shows.
I think the data is quite strong that you can safely ignore anyone who tells you that there is only one way to lose weight. If you’ve got what scientists call excess adiposity—too much fat—losing weight is a good idea for your health, but there’s no one diet that will work. My advice is to try a few and pick the one that feels easiest for you.
Intermittent fasting isn’t special, but then neither is any other diet out there.
Excellent post – thank you for breaking down the Cochrane review so clearly!
I turn to IF periodically, not for weight loss, but to help "reset" when I've started to eat too much junk. It's a psychological effect: Eating windows help me be more mindful about what I'm eating.
You mentioned that two book agents have turned down your idea that all diets are about the same for one's health. I wonder if you added (or would want to add) that each diet may have micro-benefits that depend on the individual. For instance, I imagine that IF would be no better or worse than any other diet if I were aiming for weight loss. But as for changing the content of what I eat, IF works better than anything else. I don't need a chart describing the Mediterranean diet. I need something that pushes me to think about what I eat next.
Your overall message certainly makes sense, no one diet works like magic for everyone. My quibble about the conclusion that fasting is about the same as any other calorie restriction Model is that the analysis lumps all the studies together and calls it intermittent fasting.
Fasting is just one of the methods I teach in my clinic, but I do suggest it frequently. But of course there are myriad models of IF and I strongly feel that each model needs to be evaluated separately. In my mind, for instance, the models that utilize calorie restriction to 500 calories on "fasting" days isn't fasting at all! That's just calorie restriction. Also, most studies of more traditional models focus on a 16 hour fasting window which, in my clinical experience, I rarely find works well. Jump up to a 20 hour window (with NO calorie restriction during the eating window) and success jumps up substantially. Of course clinical experience can not take the place of controlled trials, but lumping all of these "fasting" trials together even when they aren't actually having patients fast just muddies the water.